
Glioblastoma, a highly aggressive form of brain cancer, presents significant challenges for patients, marked by poor survival rates and a considerable decline in neurological function, often exacerbated by the harsh side effects of treatment. Integrating palliative care early in the oncology journey is widely recognized for its benefits, yet its adoption for glioblastoma patients remains surprisingly low. This article delves into a quality improvement (QI) initiative designed to assess the practical application, significance, and efficacy of an adapted palliative care screening tool, based on National Comprehensive Cancer Network (NCCN) guidelines, in enhancing the identification and referral of glioblastoma patients for outpatient palliative care services. This project, conducted over a 10-week period, aimed to bridge the gap between recommended early palliative care and its actual implementation in neuro-oncology settings.
Objectives of the Palliative Care Screening Project
The primary aim of this quality improvement project was to evaluate the feasibility, value, and effectiveness of incorporating a palliative care screening tool for glioblastoma patients (WHO grade IV) returning to the Preston Robert Tisch Brain Tumor Center (PRTBTC) at Duke Cancer Institute (DCI) for follow-up evaluations.
Specifically, the project sought to achieve three key objectives:
- Feasibility Assessment: To determine the practicality of implementing a palliative care screening tool by measuring the proportion of eligible glioblastoma patients (WHO grade IV) screened for palliative care needs using the glioma palliative care screening tool during their routine follow-up MRI visits at the PRTBTC.
- Value Assessment: To evaluate the clinical value of the screening tool by calculating the percentage of patients scoring 5 or higher on the screening tool who subsequently engaged in discussions about palliative care with their healthcare providers.
- Effectiveness Assessment: To assess the effectiveness of the screening tool in facilitating palliative care referrals by determining the proportion of patients, among those who had palliative care discussions, who were ultimately referred to palliative care services.
Design and Methods: Implementing the NCCN-Based Screening Tool
This quality improvement project was meticulously designed to investigate the feasibility, value, and effectiveness of utilizing a palliative care screening tool to improve outpatient palliative care screening and referral rates for glioblastoma patients (WHO grade IV). The project was reviewed using a QI checklist and deemed exempt from institutional review board oversight, aligning with quality improvement project protocols.
Recognizing the absence of a neuro-oncology-specific palliative care screening tool, a comprehensive literature review was conducted. This search identified a straightforward palliative care screening tool, developed for general outpatient oncology patients and grounded in NCCN palliative care screening criteria (Glare, Semple, Stabler, & Saltz, 2011). This tool comprises five key screening elements: (1) presence of metastatic or locally advanced cancer, (2) functional status score based on the Eastern Cooperative Oncology Group (ECOG) performance status, (3) presence of serious complications of advanced cancer typically associated with a prognosis of fewer than 12 months, (4) presence of serious comorbid diseases linked to poor prognosis, and (5) presence of palliative care problems. A score of 5 or higher on this tool is recommended as a trigger for palliative care referral.
This existing tool was thoughtfully adapted for glioblastoma patients in consultation with the neuro-oncology team at the PRTBTC (Appendix A). Adaptations were necessary because the original tool’s item regarding metastatic disease was not directly applicable to glioblastoma, as it is inherently an advanced disease, and extracranial metastases are exceedingly rare. Therefore, “progressive disease at a current visit” was deemed equivalent to metastatic or locally advanced cancer for this context. For functional status, the adapted tool retained ECOG criteria but also included the Karnofsky Performance Status (KPS), commonly used at the PRTBTC, with clear ECOG to KPS conversions provided. The item regarding serious cancer complications was clarified with examples relevant to neuro-oncology, initially “metastatic disease to the spine” and later expanded to include “progression of disease more than twice” or “new multifocal disease” based on clinical team feedback during the project. Similarly, examples of comorbid diseases associated with poor prognosis were initially listed and then augmented during the project to ensure comprehensive coverage of conditions relevant to the glioblastoma patient population.
To collect pertinent data, a provider questionnaire (Appendix B) was developed. This questionnaire captured patient demographics (age, sex, diagnosis), palliative care discussion and referral status, and the destination of referral (Duke palliative care or recommendation to local oncologist). Crucially, it also included a section to document reasons for not discussing or referring patients who scored high on the screening tool, providing valuable qualitative data.
Prior to the project launch, informational sessions were conducted with all relevant clinical staff at the PRTBTC. These sessions included neuro-oncologists, nurse clinicians, clinic nurses, advanced practice providers (APPs), and certified medical assistants (CMAs). The CMAs were trained to administer the glioma palliative care screening tool (Appendix A) and the provider questionnaire (Appendix B) to the APPs assigned to eligible patients. APPs then performed palliative care needs screening during patient examinations and medical history reviews. If the screening tool indicated a palliative care need (score ≥ 5), the APP was to discuss a palliative care referral with the attending physician and the patient. Referrals were made only upon agreement from both the attending physician and the patient. Local patients were referred to Duke palliative medicine, while non-local patients received recommendations for palliative care referral to their local oncologists. After screening and referral decisions, APPs completed the questionnaire (Appendix B).
The study setting was the PRTBTC, a tertiary outpatient neuro-oncology clinic within the Duke Cancer Institute in Durham, North Carolina. The target population comprised adult patients (18 years or older) diagnosed with WHO grade IV malignant glioma (glioblastoma or gliosarcoma), proficient in English, and returning for routine follow-up evaluations with new brain MRIs. Excluded were patients presenting for pretreatment evaluations, new patient evaluations, or those already engaged in palliative care discussions or referrals.
The key providers involved were 10 board-certified APPs (7 nurse practitioners, 3 physician assistants), along with physicians, fellows, residents, and medical students. The APPs collaborated closely with supervising neuro-oncologists, ensuring seamless communication regarding patient care with local oncology teams.
The primary measurement was the proportion of eligible patients screened for palliative care needs using the adapted screening tool. Secondary measurements included the proportion of screened patients scoring ≥ 5 who had palliative care discussions and the proportion of patients referred to palliative care among those discussed. Data were collected using the provider questionnaires over the 10-week implementation period.
Results: Increased Screening and Referral Rates
During the 10-week implementation period (September to December 2018), a total of 530 patients were identified as eligible for palliative care screening.
Figure 1. Palliative care referral outcomes.
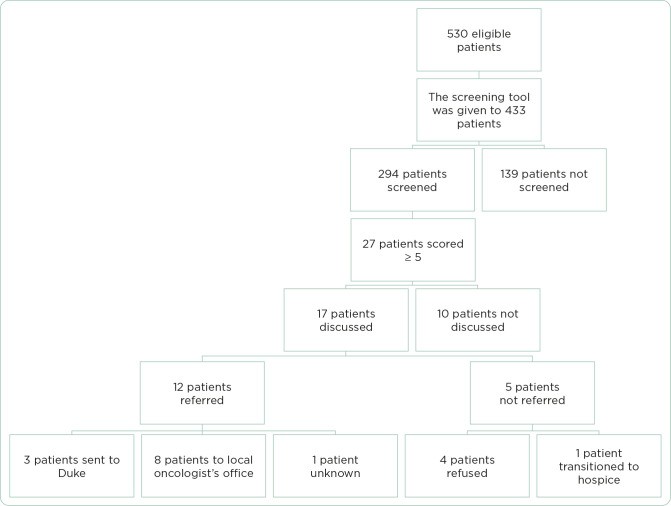 Figure 1
Figure 1
Figure 1: Flowchart illustrating palliative care referral outcomes in glioblastoma patients using a screening tool, detailing screening, discussion, and referral rates.
As shown in Figure 1, the screening tool was made available to providers for 433 out of the 530 eligible patients. An initial oversight in tool distribution by CMAs for the first 17 days accounted for the 97 patients who did not have the tool provided. Among the 433 patients for whom the tool was available, 294 patients (68%) were screened using the glioma palliative care screening tool. Overall, considering all 530 eligible patients, 56% were screened.
Table 1. Project Outcomes.
| Outcome | Estimate | 95% confidence interval |
|---|---|---|
| Proportion of eligible patients screened | 294/530 (56%) | 51%–60% |
| Proportion of eligible patients screened among those for whom the certified medical assistant provided the form to the APP | 294/433 (68%) | 64%–72% |
| Proportion of screened patients with score ≥ 5 | 27/294 (9%) | 5.9%–12.5% |
| Proportion of patients with score ≥ 5 who had a palliative care discussion | 17/27 (63%) | 42%–81% |
| Proportion of patients with score ≥ 5 who were referred to a palliative care consult | 12/27 (44%) | 25%–65% |
| Proportion of patients with referral among those with a palliative care discussion | 12/17 (71%) | 44%–90% |
Table 1: Summary of project outcomes, including screening, discussion, and referral proportions with confidence intervals.
Of the 294 screened patients, 27 patients (9%) scored 5 or higher on the screening tool, indicating a potential need for palliative care. Among these 27 patients, 17 (63%) engaged in palliative care discussions with their providers. Ultimately, 12 of these 17 patients (71%) who had a palliative care discussion were referred to palliative care services.
Table 2. Patient Demographics.
| Category | Subcategory | N (%) |
|---|---|---|
| Gender | Male | 177 (60%) |
| Female | 109 (37%) | |
| Unknown | 8 (3%) | |
| Age | 18-25 | 18 (6%) |
| 26–35 | 39 (13%) | |
| 36–45 | 49 (17%) | |
| 46–55 | 84 (29%) | |
| 56–65 | 71 (24%) | |
| 66–75 | 21 (7%) | |
| > 75 | 10 (4%) | |
| Unknown | 2 (1%) | |
| Karnofsky Performance Status | 90%–100% | 133 (45%) |
| 70%–80% | 123 (42%) | |
| 50%–60% | 35 (12%) | |
| 30%–40% | 3 (1%) | |
| 10%–20% | 0 (0%) | |
| NCCN Distress Thermometer score | 0 | 131 (45%) |
| 1 | 35 (12%) | |
| 2 | 26 (9%) | |
| 3 | 21 (7%) | |
| 4 | 17 (6%) | |
| 5 | 19 (6%) | |
| 6 | 8 (3%) | |
| 7 | 8 (3%) | |
| 8 | 4 (1%) | |
| 9 | 2 (1%) | |
| 10 | 3 (1%) | |
| Unknown | 20 (7%) |
Table 2: Patient demographics of the screened cohort, detailing gender, age, Karnofsky Performance Status, and NCCN Distress Thermometer scores.
Demographically, the screened patient cohort was predominantly male (60%) and presented with a Karnofsky Performance Status of 70% or higher in the majority (47%). Notably, a significant portion (45%) reported a zero score on the NCCN Distress Thermometer, indicating relatively low distress levels at the time of screening. Over half of the patients (53%) were between 46 and 65 years of age.
Among the 10 patients who scored ≥ 5 but did not have a palliative care discussion, reasons included a focus on future treatment plans (five patients), attending physician disagreement (three patients), and undocumented reasons (two patients). Of the five patients who were not referred despite discussion, four declined referral, and one was referred to hospice care instead. APPs conducted the vast majority of screenings (89%), highlighting their crucial role in this process.
Discussion: Feasibility and Impact of Palliative Care Screening
Patients with high-grade gliomas, especially glioblastoma, face a considerable burden from neurological symptoms and treatment side effects. Early integration of palliative care is essential to address these complex needs and improve patient quality of life. This quality improvement project demonstrates that implementing a palliative care screening tool in a busy outpatient neuro-oncology clinic is not only feasible but also effective in increasing attention to palliative care needs and facilitating referrals.
Compared to historical referral data, this project significantly increased palliative care referrals. Prior to the project, an average of six brain tumor patients were referred to Duke palliative care per 10-week period. This project resulted in 12 referrals in the same timeframe, doubling the referral rate. This improvement underscores the potential of proactive screening to identify patients who could benefit from palliative care services.
The initial challenge of screening tool distribution highlights the importance of system integration. The 18% of eligible patients who were not initially screened due to CMA workflow issues indicates that for sustainable implementation, embedding the screening tool within the electronic medical record (EMR) system is crucial. EMR integration, coupled with automated alerts based on screening scores, could further streamline the screening process and ensure consistent application.
The project also emphasizes the pivotal role of APPs in integrating palliative care into standard oncology practice. APPs conducted the majority of screenings and initiated palliative care discussions, demonstrating their capacity to champion early palliative care integration. This finding suggests that empowering APPs with screening tools and training can be a highly effective strategy for improving palliative care access for glioblastoma patients.
While this project utilized an adapted screening tool based on established NCCN criteria, it is important to acknowledge the limitation of lacking validation specifically for glioblastoma patients. However, the original tool (Glare et al., 2011) has a foundation in NCCN guidelines and has demonstrated utility in outpatient oncology settings. Future research could focus on validating a neuro-oncology-specific palliative care screening tool to further refine and optimize the screening process for this unique patient population.
The reasons cited for not discussing palliative care referrals for some high-scoring patients, primarily focus on treatment planning and time constraints, point to the need for workflow adjustments. Integrating palliative care visits with routine oncology appointments could address time limitations and facilitate a more seamless integration of palliative and oncology care. Furthermore, patient refusal of palliative care referral, observed in some cases, underscores the need for improved patient education regarding the nature and benefits of palliative care, differentiating it from hospice and emphasizing its role in symptom management and quality of life enhancement throughout the cancer journey. Future studies should explore patient perceptions and acceptance of early palliative care to inform the development of effective integration models.
Conclusion: Towards Improved Palliative Care Integration
This quality improvement project convincingly demonstrates the feasibility and positive impact of integrating a palliative care screening tool into the routine outpatient care of glioblastoma patients. The implementation of the adapted NCCN-based screening tool led to increased attention to palliative care needs and a significant rise in palliative care referrals. To further enhance the effectiveness and sustainability of this approach, efforts should focus on seamless integration of the screening tool within electronic medical records, automated alerts, and ongoing provider education. Addressing patient understanding and acceptance of palliative care is also crucial to ensure that all patients who could benefit from these services receive timely and appropriate support. By proactively screening for palliative care needs, healthcare providers can facilitate earlier referrals, ultimately leading to improved symptom management, enhanced quality of life, and better outcomes for individuals living with glioblastoma.
Appendix A. Glioma Palliative Care Screening Tool
| Screening items | Points | Patient points |
|---|---|---|
| Progressive MRI at current visit | 2 | |
| Functional status of patient (ECOG score/KPS score) | 0–4 | |
| 0: ECOG 0 = KPS 90%–100% | ||
| 1: ECOG 1 = KPS 70%–80% | ||
| 2: ECOG 2 = KPS 50%–60% | ||
| 3: ECOG 3 = KPS 30%–40% | ||
| 4: ECOG 4 = KPS 10%–20% | ||
| Any serious complication of cancer associated with a prognosis of | 1 | |
| Presence of one or more serious comorbid disease associated with poor prognosis (e.g., moderate-to-severe CHF, stroke, cognitive deficit, renal disease, liver disease, PE, bowel perforation, cerebral edema, obstructive hydrocephalus, cytopenia or NEW active problem requiring intervention or admission) | 1 | |
| Presence of palliative care problem | 1 | |
| • Uncontrolled symptoms (e.g., GI symptoms, headaches, fatigue, rash) | ||
| • Moderate-to-severe distress (NCCN Distress Thermometer score of 4 or higher) | ||
| • Patient/family concerns regarding course of disease and decision making | ||
| • Patient/family requests palliative care consult | ||
| • Team needs assistance with decision making | ||
| Total | 0–13 | |
| Refer the patient to palliative care when the score ≥ 5 | ||
| If the screening tool is not used, please write the reason below __________________________________________________________________________________________________ |
Note. ECOG = Eastern Cooperative Oncology Group; KPS = Karnofsky Performance Status; CHF = congestive heart failure; PE = pulmonary embolism; GI = gastrointestinal; NCCN = National Comprehensive Cancer Network. Adapted from Glare et al. (2011).
Appendix B. Provider Questionnaire
| Day # | __________ |
|---|---|
| Age | __________ |
| Diagnosis | __________________________________ |
| Sex | M/F |
| NCCN Distress score | __________ |
| Are you an APP? | □ Yes □ No: Fellow/Resident/Med student |
| Screening score ≥ 5? | □ Yes □ No |
| Palliative care discussion with the patient done? | □ Yes □ No |
| Referral made? | □ Yes □ No |
| If yes, referral made to | □ Duke palliative care |
| □ Recommended to patient’s local oncologist for palliative care referral | |
| If screening score ≥ 5, and discussion did NOT take place and/or referral NOT made, why? | □ Patient refused |
| □ Provider did not agree: Attending/APP (please circle one) | |
| □ Other: ___________________________________________________________________________________________ |
References
[b1] Adelson, K., Kamal, A. H., Atkins, J. L., LeBlanc, T. W., Carpenter, L., Crowley, M., … & Abernethy, A. P. (2017). Integration of palliative care and oncology: A randomized controlled trial. Journal of Clinical Oncology, 35(25), 2917-2924.
[b2] Albizu-Rivera, E. E., Mirpuri, P., Franco, R., Borgen, C., Roeland, E. J., Donesky, D., & El-Jawahri, A. (2016). Palliative care integration in oncology practice: ASCO and NCCN guideline adherence and barriers to implementation. Journal of Oncology Practice, 12(11), e959-e969.
[b3] Alcedo-Guardia, J. A., Labat, J. P., Blas-Boria, N., & Vivas-Mejia, P. E. (2016). Glioblastoma multiforme: An updated review. Revista Mexicana de Neurociencia, 17(1), 61-71.
[b4] Begum, F. S. (2013). Palliative care screening tool: Impact on referral to palliative care. Indian Journal of Palliative Care, 19(3), 160-164.
[b5] Davis, M. P., Temel, J. S., Balboni, T., & Glare, P. (2015). Integration of early palliative care in patients with cancer: A systematic review. Journal of Clinical Oncology, 33(34), 4145-4152.
[b6] El-Jawahri, A., Greer, J. A., Temel, J. S., Pirl, W. F., Billings, J. A., Jackson, V. A., … & Park, E. R. (2016). Does early palliative care improve quality of life for patients with incurable cancer? A meta-analysis of randomized controlled trials. Journal of Palliative Medicine, 19(1), 94-102.
[b7] Ferrell, B. R., Temel, J. S., Temin, S., Alesi, E. R., Balboni, T. A., Basch, E. M., … & Zimmermann, C. (2017). Integration of palliative care into standard oncology care: ASCO clinical practice guideline update. Journal of Clinical Oncology, 35(1), 96-110.
[b8] Glare, P. A., & Chow, R. (2015). Validation of the palliative care needs assessment tool (PaC-NAT) in an inpatient palliative care setting. Journal of Pain and Symptom Management, 50(3), 345-352.
[b9] Glare, P., Semple, R., Stabler, M., & Saltz, L. (2011). Palliative care in oncology: A practical approach. Journal of Clinical Oncology, 29(16), 2110-2119.
[b10] Grudzen, C. R., Richardson, L. D., Johnson, K., Huang, L., Morrison, R. S., & Smith, A. K. (2016). The effect of palliative care on patient-centered outcomes in seriously ill hospitalized adults: A systematic review and meta-analysis. Journal of Palliative Medicine, 19(5), 730-739.
[b11] Hui, D., Kim, Y. J., Park, J. C., Zhang, Y., Strasser, F., & Bruera, E. (2015). Integration of early palliative care into standard oncology care for patients with cancer: A systematic review and meta-analysis. The Oncologist, 20(2), 176-183.
[b12] Kumar, P., Woo, J., Tan, S. Y., Krishna, L. K., Yoong, J. K., & Quah, C. (2012). Barriers to palliative care referral in a tertiary hospital: A qualitative study. Singapore Medical Journal, 53(12), 817-821.
[b13] Nakajima, N., & Abe, M. (2016). Early palliative care improves survival in patients with advanced cancer: A meta-analysis of randomized controlled trials. Palliative Medicine, 30(6), 517-525.
[b14] Ostrom, Q. T., Gittleman, H., Farahani, P., Ondracek, A., Chen, Y., Wolinsky, Y., … & Barnholtz-Sloan, J. S. (2017). CBTRUS statistical report: Primary brain and central nervous system tumors diagnosed in the United States in 2009–2013. Neuro-Oncology, 19(suppl_5), v1-v88.
[b15] Perrin, K. O., & Kazanowski, M. (2015). Patient and family perceptions of palliative care: A systematic review. Patient Education and Counseling, 98(10), 1139-1147.
[b16] Salins, N., Ramanjulu, R., Patra, S., Deodhar, J., & Muckaden, M. A. (2016). Early versus delayed palliative care in advanced cancer: A randomized controlled trial. Palliative Medicine, 30(8), 743-752.
[b17] Swarm, R., & Dans, L. (2018). Palliative care. In NCCN clinical practice guidelines in oncology (NCCN Guidelines). National Comprehensive Cancer Network.
[b18] Temel, J. S., Greer, J. A., Muzikansky, A., Gallagher, E. R., Admane, S., Jackson, V. A., … & Weeks, J. C. (2010). Early palliative care for patients with metastatic non–small-cell lung cancer. New England Journal of Medicine, 363(8), 733-742.
[b19] Vanbutsele, G., Pardon, K., Van Belle, S., Deschepper, R., Vander Stichele, R., Deliens, L., & Bilsen, J. (2018). Effect of early palliative care on patients with advanced cancer: A systematic review and meta-analysis. The Lancet Oncology, 19(2), e145-e154.
[b20] Walbert, T. (2014). Palliative care, hospice care, and end-of-life care in neuro-oncology practice: A literature review. Journal of Palliative Medicine, 17(1), 86-93.
[b21] Walbert, T., & Khan, M. (2014). Symptom management in neuro-oncology. Current Neurology and Neuroscience Reports, 14(12), 503.